I had the privilege of presenting in this thematic area for the Shanghai Forum and addressed the priority for prevention. This contrasted with a preceding talk that advocated for greater emphasis on genomic testing to focus prevention activities within the Chinese population. Using diabetes and breast cancer examples I contrasted the time course of disease development and the importance of acting now with our current information, particularly given the dramatic changes in diet and physical activity among children in China over the past 25 years. Needless to say, diet has moved to more western pattern increasing risk of diabetes and cancer, physical activity has declined.
The immediacy of providing health services makes demands on health systems that draw the focus away from using the knowledge we already have. Lets look at the evidence on breast cancer as an example of why we need to act quickly to reduce the global burden. Already, breast cancer is the number 1 cancer diagnosis among women in the world. In 2012, 1.7 million women were diagnosed with breast cancer (25% of all new cancer cases).
In Asia the incidence rate of breast cancer in women under age 50 continues to rise. For example, data from the shanghai tumor registry included in the IARD report on cancer are summarized below.
|
35-39
|
40-44
|
45-49
|
|
|
1998-2002
|
32.0
|
76.5
|
104.4
|
|
1993-1997
|
35.6
|
60.6
|
86.9
|
|
1988-1992
|
31.5
|
61.1
|
81.5
|
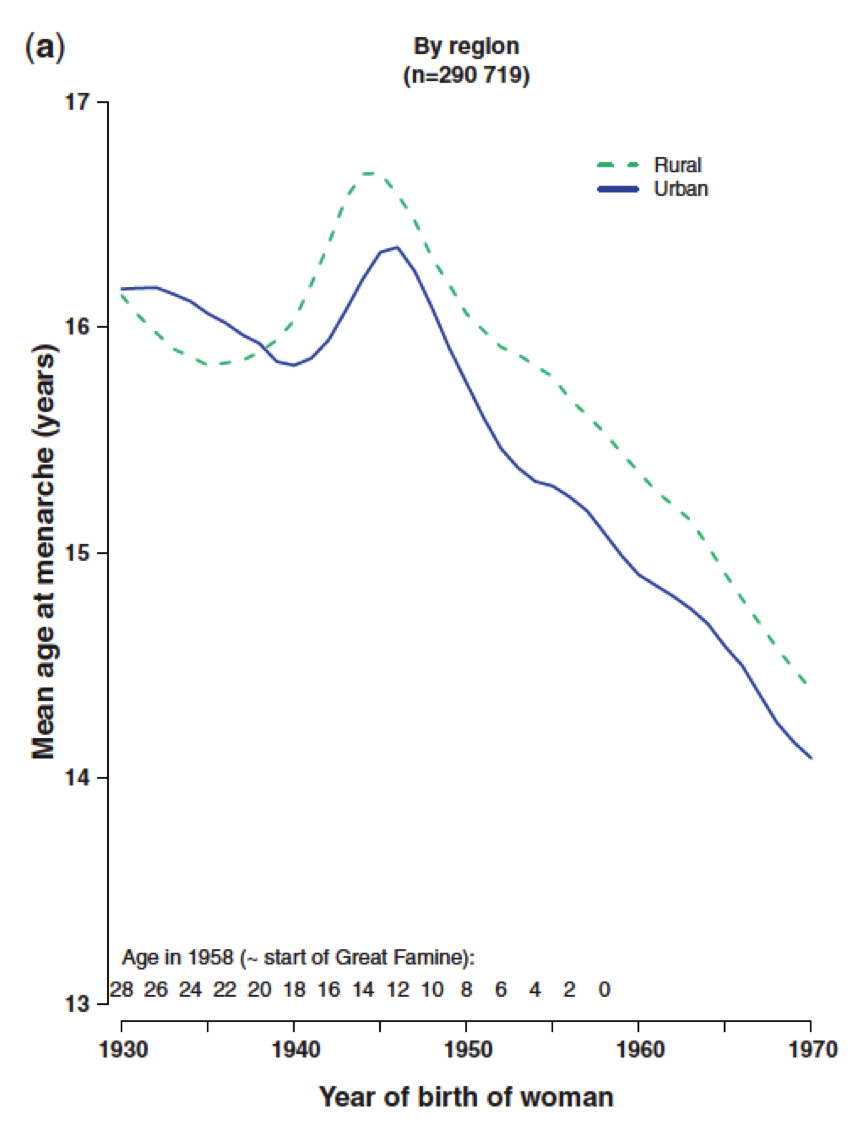
This is no surprise because age at first menstrual period has fallen from an average of 16 or 17 for women born in 1930 to 14 for women born in 1970 1 and down to 12 for women born in Beijing by 1990 (menarche assessed through 2004). This age at menarche is slightly younger in cities and a little older for those in rural settings.
Figure 1. Age at menarche by year of birth for women in China from Lewington et al IJE 2014.
The number of children has plummeted throughout the world. Although the number of babies born continues to rise to a possible record of 136 million babies in 2007 (May 23, 2014: http://www.worldwatch.org/node/5645). This is explained by the number of women between age 15 and 49, which has double in the past 435years, to 1.7 billion. Thus, even with fewer babies born for each women, the total births rise and global population is projected to pass beyond 9 billion, stressing our ability to feed and provide health services for all.
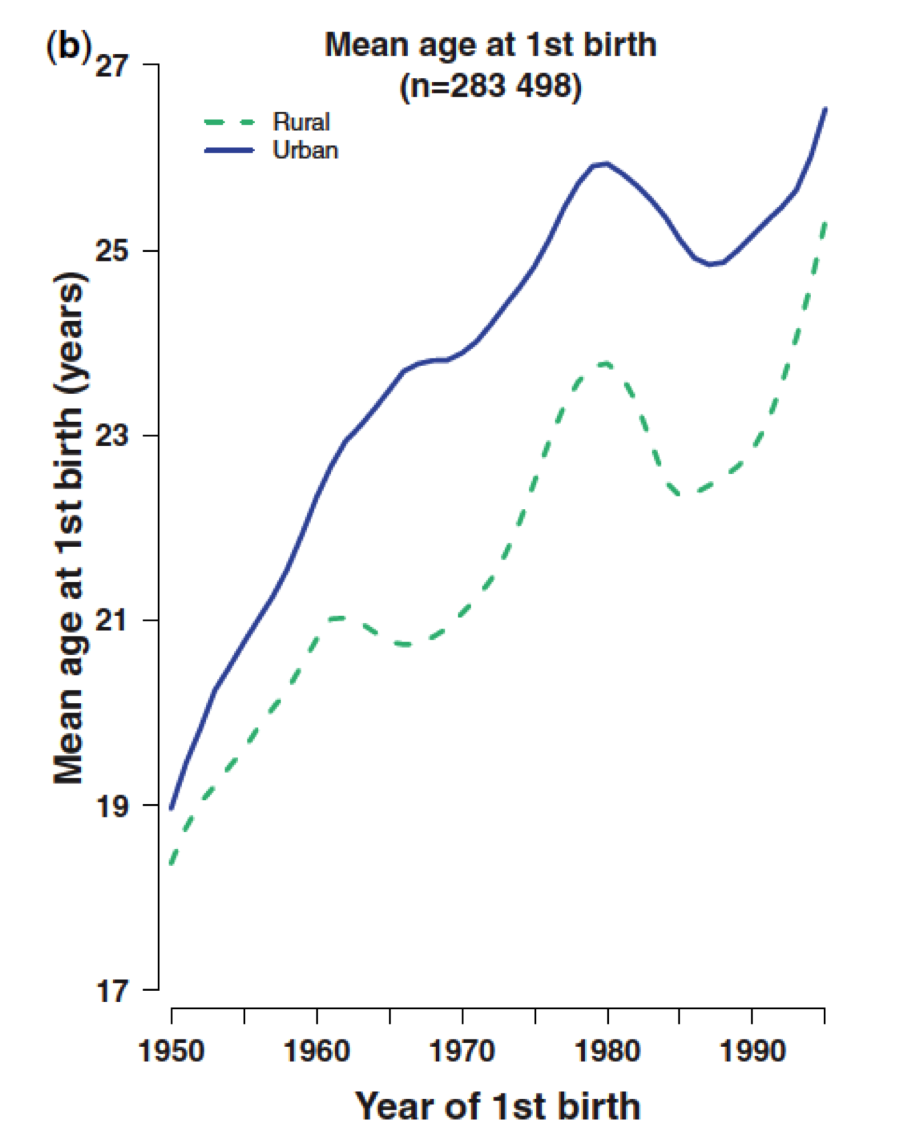
Back to number of children… in China up to 1950 women had an average of 5 babies (urban) or 6 children (in rural settings) – see figure 2, ale drawing on Lewington et al IJE 2014.

The age a women has her first baby has increased from 19 in 1950 to 25 or more in 1995.
Children historically were spaced about 3 years apart and this has increased in the recent past of those who have more than 1 child.
Based on one survey of several hundred thousand women, …
As a society or civilization, we have effectively extended the interval from first menstrual period to first birth from about 2 years to almost 18. This given an increase in the number of menstrual periods on average before first birth from say fewer than 26 menstrual periods; to some 234 cycles (18yrs x13 cycles/year), before the full cellular differentiation that accompanies breast development during first pregnancy; this is an increase of more than 200 cycles. Furthermore, it represents almost 18 more years of breast risk accumulation before the protection of first pregnancy. Lifestyle during this time of life determines life long risk of breast cancer.
Using our validated model of breast cancer incidence 2,3 we know that, if a woman has a first baby at 19 and has the weight and height of average women in China born 1925 to 1978 4 then at age 50 she would have an incidence rate of about 50 cases per 100,000 women. In contrast the current incidence in the USA is 182 cases per 100,000 women (SEER data).
If, however, we apply the new normal, menarche at 12, first birth at 27, and only 1 birth (consistent with China and Korea today) then we expect an incidence of about 147 cases per 100,000 women at age 50. The current incidence in Korea closely reflects these numbers, as do data from Shanghai. Shifting patterns of reproductive characteristics of women in a population dramatically change breast cancer incidence.
So what are we ignoring?
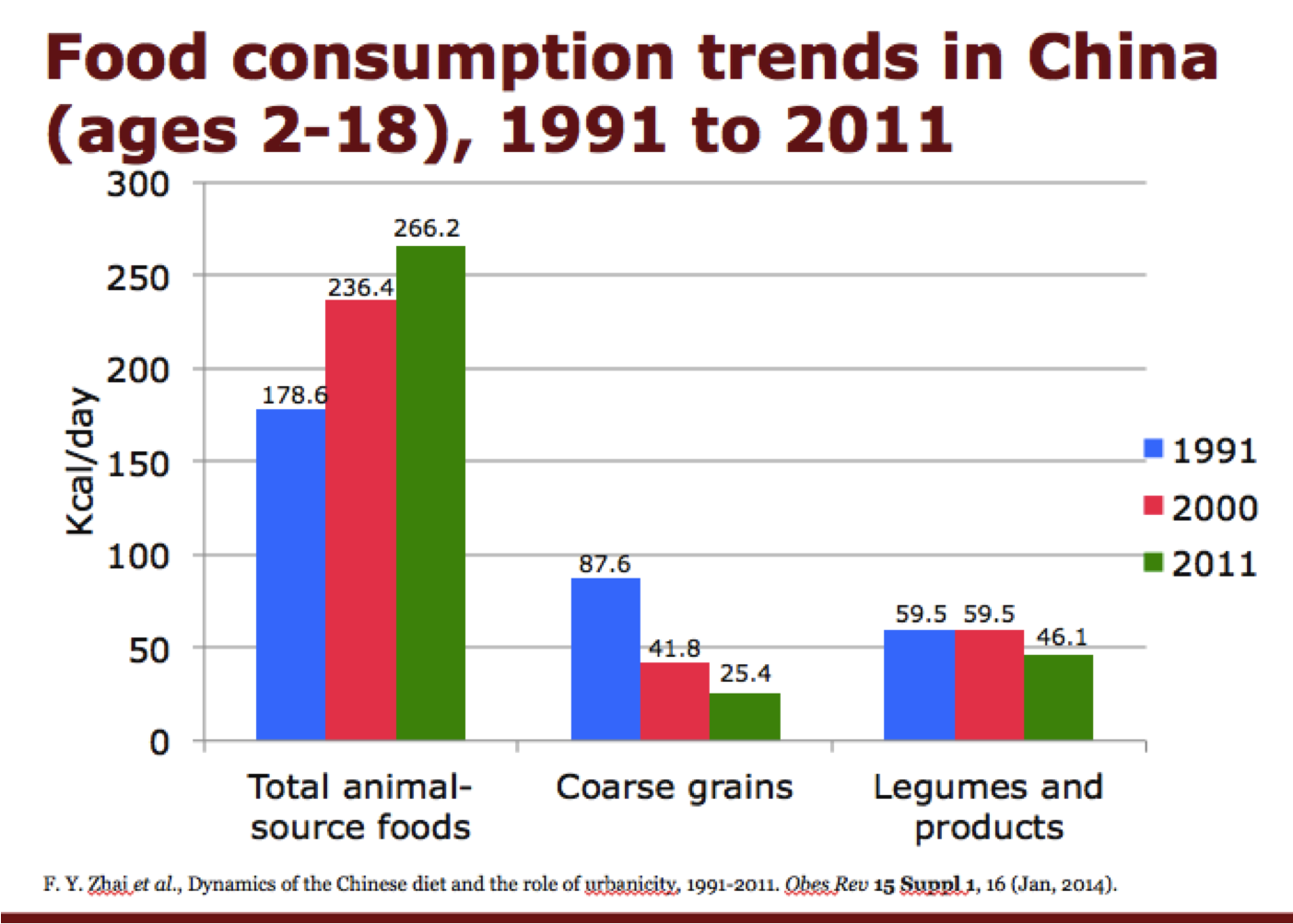
Strong evidence supports higher intake of vegetables in the diet are related to lower risk of breast cancer. Soy intake in childhood and adolescence is related to lower risk 5-7, as is higher fiber intake 8 and higher vegetable protein intake 8-10. Yet, China has had a hugged drop in consumption of vegetable sources in the diet and greatly increased intake of animal sources. The data from the China National Health Survey for children 2 to 18 years of age are summarized in the figure. We note a 50% increase in animal sources and a 70% decrease in course fiber sources in the diet over the 120 years form 1991 to 2011 11.
Physical activity in adolescence is directly related to lower risk of breast cancer 12,13 – yet we see continuing trends with industrialization to lower physical activity. Driven largely by a drop in occupational activity women in china have decreased their overall activity by about 50% from 1991 to 2011 14.
These dietary changes and reductions in physical activity will combine to exacerbate the increase in risk driven by changing reproductive patterns.
Of course, with higher education we see women drinking more alcohol.
In China, for example, women without high school education report abstaining from alcohol. Based on data from 500,000 men and women enrolled in the China Kadoorie Biobank cohort study born 1925 to 1978; overall 63% of women reported never drinking alcohol 15. When stratified by education alcohol consumption increased with level of education. Among women with no formal education 71% never drank alcohol, while for women with college or university education, 47.8 % never drank. Alcohol a known breast carcinogen is increasing and will add further to the burden of breast cancer. Importantly, intake between first menstrual period and first birth drives risk of premalignant and invasive breast lesions 16,17.
Recommendations
While the world health organization recommends not smoking, eating a healthy diet, being physically active, and limiting alcohol intake, the importance of age is ignored18. For beast cancer, the leading cancer burden among women in the world, we must refocus on the critical period before age 30 when breast cells are most susceptible to risk and lifetime risk is set.
If we act and act now, supported by additional resources devoted to implementing prevention, bringing messages and sustaining lifestyle and risk reduction strategies during the critical time points in life, we can achieve a world-wide turn around overcoming outrage. The burden of the leading cancer diagnosed in women can decrease now and for future generations.
Literature cited
1. Lewington S, Li L, Murugasen S, et al. Temporal trends of main reproductive characteristics in ten urban and rural regions of China: the China Kadoorie Biobank study of 300 000 women. Int J Epidemiol. Mar 17 2014.
2. Rosner BA, Colditz GA, Hankinson SE, Sullivan-Halley J, Lacey JV, Jr., Bernstein L. Validation of Rosner-Colditz breast cancer incidence model using an independent data set, the California Teachers Study. Breast cancer research and treatment. Nov 2013;142(1):187-202.
3. Colditz GA, Rosner B. Cumulative risk of breast cancer to age 70 years according to risk factor status: data from the Nurses’ Health Study. American journal of epidemiology. Nov 15 2000;152(10):950-964.
4. Chen Z, Chen J, Collins R, et al. China Kadoorie Biobank of 0.5 million people: survey methods, baseline characteristics and long-term follow-up. Int J Epidemiol. Dec 2011;40(6):1652-1666.
5. Wu AH, Yu MC, Tseng CC, Pike MC. Epidemiology of soy exposures and breast cancer risk. Br J Cancer. Jan 15 2008;98(1):9-14.
6. Korde LA, Wu AH, Fears T, et al. Childhood soy intake and breast cancer risk in Asian American women. Cancer Epidemiol Biomarkers Prev. Apr 2009;18(4):1050-1059.
7. Yang G, Shu XO, Li H, et al. Prospective cohort study of soy food intake and colorectal cancer risk in women. Am J Clin Nutr. Feb 2009;89(2):577-583.
8. Liu Y, Colditz GA, Cotterchio M, Boucher BA, Kreiger N. Adolescent dietary fiber, vegetable fat, vegetable protein, and nut intakes and breast cancer risk. Breast cancer research and treatment. Apr 16 2014.
9. Berkey CS, Willett WC, Tamimi RM, Rosner B, Frazier AL, Colditz GA. Vegetable protein and vegetable fat intakes in pre-adolescent and adolescent girls, and risk for benign breast disease in young women. Breast cancer research and treatment. Sep 2013;141(2):299-306.
10. Su X, Tamimi RM, Collins LC, et al. Intake of fiber and nuts during adolescence and incidence of proliferative benign breast disease. Cancer causes & control : CCC. Jul 2010;21(7):1033-1046.
11. Zhai FY, Du SF, Wang ZH, Zhang JG, Du WW, Popkin BM. Dynamics of the Chinese diet and the role of urbanicity, 1991-2011. Obes Rev. Jan 2014;15 Suppl 1:16-26.
12. Bernstein L, Henderson BE, Hanisch R, Sullivan-Halley J, Ross RK. Physical exercise and reduced risk of breast cancer in young women. J Natl Cancer Inst. 1994;86:1403-1408.
13. Maruti SS, Willett WC, Feskanich D, Rosner B, Colditz GA. A prospective study of age-specific physical activity and premenopausal breast cancer. Journal of the National Cancer Institute. May 21 2008;100(10):728-737.
14. Ng SW, Howard AG, Wang HJ, Su C, Zhang B. The physical activity transition among adults in China: 1991-2011. Obes Rev. Jan 2014;15 Suppl 1:27-36.
15. Millwood IY, Li L, Smith M, et al. Alcohol consumption in 0.5 million people from 10 diverse regions of China: prevalence, patterns and socio-demographic and health-related correlates. Int J Epidemiol. Jun 2013;42(3):816-827.
16. Liu Y, Tamimi RM, Berkey CS, et al. Intakes of alcohol and folate during adolescence and risk of proliferative benign breast disease. Pediatrics. May 2012;129(5):e1192-1198.
17. Liu Y, Colditz GA, Rosner B, et al. Alcohol intake between menarche and first pregnancy: a prospective study of breast cancer risk. Journal of the National Cancer Institute. Oct 16 2013;105(20):1571-1578.
18. World Health Organization. Global Action Plan for Prevention and Control of Noncommunicable Diseases, 2013-2020. http://www.who.int/cardiovascular_diseases/15March2013UpdatedRevisedDraftActionPlan.pdf:World Health Organization,; MArch 15, 2013 2013.